PAST PROJECT
The Integrated Care for Kids (InCK) Model is led by the Centers for Medicare and Medicaid Innovation (CMMI) and Centers for Medicare & Medicaid Services (CMS). The InCK Model is a child-centered local service delivery and state payment model that aims to reduce expenditures and improve the quality of care for children under 21 years of age covered by Medicaid through: 1) Prevention, 2) Early identification, and 3) Treatment of behavioral and physical health needs.
Oregon was one of eight Integrated Care for Kids (InCK) cooperative agreement recipients.
Oregon Participated in the InCK Model from 2020-2022.
- This document summarized common questions and answers from the Oregon Health Authority on why Oregon only participated from 2020-2022.
- In early Fall 2021, the Oregon team received clarifications from the federal funder regarding the InCK Model and their expectations. A number of these clarifications required significant changes to the Oregon InCK Model and reporting requirements for 2022 that the collective teams felt were not viable to implement. OHA and OPIP made significant efforts to communicate our concerns about program viability to CMMI over the course of 2021. All grantees submitted similar concerns through formal letters jointly to CMMI leadership and held an all-grantee meeting with CMMI leadership. CMMI responded that key model design aspects and reporting requirements could not be changed due to their evaluation design.
- Oregon’s original proposal leveraged child health complexity data and infrastructure to assess needs for children and youth and communicate that information to the Coordinated Care Organization (CCO) and regional partners. We planned to use CMMI funding to implement an infrastructure to share these data and provide deep technical assistance and other resources dedicated to improving coordination and integration of services for children and their families. It then became clear we would not be able to operationalize our proposal given CMMI requirements. Given these circumstances, the Oregon team made the difficult decision to notify the federal funder that Oregon would not be applying for continuation of the InCK model in Oregon starting in 2022 and the effort ended 12/31/22.
Overview of Oregon’s InCK Model 2020-2022
The Oregon Health Authority (awardee) and the Oregon Pediatric Improvement Partnership (OPIP; sub-awardee and “Lead Organization”) jointly applied for InCK Model funding to be implemented in partnership with regional child care services partners and local CCOs in the target regions of Crook, Deschutes, Jefferson, Marion and Polk counties.
Goals: The goals are InCK were to: 1) Improve performance on priority measures of child health, 2) Reduce avoidable inpatient states and out of home placements, and the 3) Creation of sustainable Alternative Payment Models.
InCK Model Region in Oregon – The InCK Model built on CCO 2.0 key goals, regional partnerships and existing infrastructure with the following goal: The InCK Model region will focus on all Medicaid/CHIP enrolled children in Crook, Deschutes, Jefferson, Marion and Polk counties, through the following:
- Early identification of children with specific health needs
- Integrated care coordination and case management
- Health information exchange
- Development and Implementation of Alternative Payment Models (APM)
Community Level Partnerships – Community-level partnerships were critical to Oregon’s InCK model. Local CCOs in the InCK Model region, regional Partnership Councils, and local Child Core Services Providers were key to the planning, implementation, and operationalization of the InCK Model. Core services providers included clinical care (physical and behavioral), schools, early care and education, Title V, child welfare, mobile crisis response services, organizations that provide food and housing and others that addressed factors that impact a child health and health care use. Oregon’s InCK model engaged existing parent and youth voices in each region. Lastly, specific efforts were led with the Office of Health Equity to ensure partnerships are established with racial and ethnic communities most impacted by health inequities.
Summary of Oregon’s InCK Model
- Two-Page Summary
- Overview Visual of Oregon’s InCK Model
- System-Navigator: A key position of focus within the InCK model was the presence of a System-Navigator. This slide summarizes the priority roles and responsibility of the System Navigator that were confirmed and prioritized by the Partnership Councils in each region.
Distillation of Learnings from 2020-2022 Provided to Oregon Health Authority
- OPIP’s Learning as they Relate to Health Complexity
- OPIP’s Learning as They Relate to Quality Metrics and Performance Improvement Projects
- OPIP’s Learning as They Relate to Behavioral Health and Care Coordination
- OPIP’s Learnings as They Relate to Traditional Health Workers
- OPIP’s Learnings as They Relate to HIE/CIE
- OPIP Learnings as They Relate to Alternative Payment Methods
Parent, Youth and Young Adult Advisory Committee
- Oregon Integrated Care for Kids Parent, Youth and Young Adult Advisory Group: Summary of Input Collected in 2020 and 2021
INCK Partnership Council Members, Slides and Materials from Late 2020-2021
Marion and Polk Partnership Council
- Summary of December 2020 Community Café
- March 2021 Partnership Council Meeting – Summary and Slides
- June 2021 Partnership Council Meeting – Summary and Slides
- December 2021 Final Partnership Council Meeting – Summary and Slides
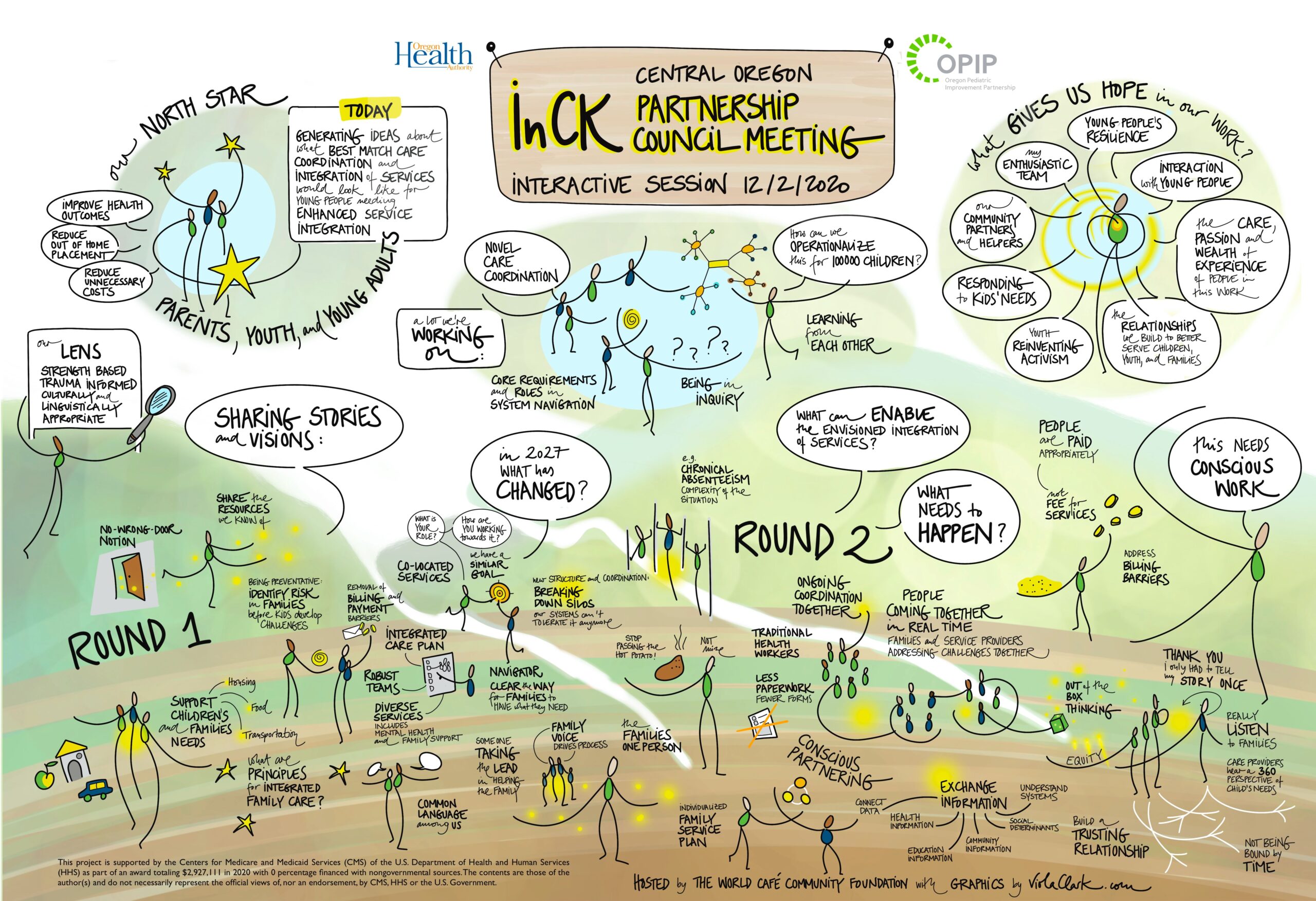
Central Oregon Partnership Council
- Summary of December 2020 Community Café
- March 2021 Partnership Council Meeting – Summary and Slides
- June 2021 Partnership Council Meeting – Summary and Slides
- December 2021 Final Partnership Council Meeting – Summary and Slides
{kind=link}
Questions? Need more information?
Contact OPIP’s Director and Lead of the OPIP Subaward Colleen Reuland at reulandc@ohsu.edu or 503-494-0456.
Acknowledgement of Funding that Supported InCK
This project from 2020-2022 was supported by Funding Opportunity Number CMS2B2-20-001 from the U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services.
Disclaimer: This project is supported by the Centers for Medicare and Medicaid Services (CMS) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $5,866,192 with 100 percentage funded by CMS/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by CMS, HHS or the U.S. Government.